Step up

In early 2011, I moved to Liberia in attempt to use my skills as a doctor and adult person to impact the welfare and lives of people hit by war, pathogens, bad leaders and the like. From Liberia I headed to Indonesia and then when Ebola hit, I returned to Liberia again. I was filled with excitement. I was new to the field of international health and felt it was time to leave the bureaucracy of the NYC Department of Health before petrification of spirit. I had just proposed to Seongeun. I knew Monrovia was not a place for the meek. And I was joining an organization whose reputation made a 50% pay cut seem like a deal. I truly felt that the entire world was before me. Later students would ask what it felt like to make so little money while putting my personal welfare at risk and I would scold them for their arrogance and entitlement. I have never regarded work as a sacrifice. Being regularly paid to take care of people is the best possible excuse for this liberal. Also, I am pretty sure most people in the world don’t get to live next to the ocean— Monrovia, watch cows silhouetted by the rising soon as they bathe— Kirehe, or be driven around in a Jeep—Everywhere there is mud.
What would one buy anyway in Liberia? Mango’s? I seriously saved everything. I ponder this potentially offensive and defensive line of thinking six years later, as I sit in a soon to be decommissioned 747 (Note to Delta HQ: No need to announce this detail) roaring towards South East Asia-- a 27 hour flight. Much is different now. I have too many gray hairs to pluck. Seongeun and I have a beautiful daughter who is nineteen months old going on three years, who cried no no no so many times when I left that she made me want to cry. My basketball game is seriously better (the advantages of not having to play on a dirt court). I am not going away to live.

Travel away from Drew is a surprisingly hard. I never thought I'd feel this way
Yet much is similar. The route is as long and circuitous: JFK to DTW to Narita to Singapore to Bangkok to Jakarta to Medan. Travel thru West Africa could be halted at any moment by a functionary suddenly declaring that one’s paid flight had been cancelled (until $100 made it un-cancelled). When I left New York City, the Delta representative at the counter told me that because my passport would expire within six months of my return flight, I could not board the plane (unless I bought an earlier ticket back, which I then cancelled). Later, I sat next to a Filipino man who was not Ghanaian but who also introduced me to Christ. I still love mangos and am willing to travel anywhere in the world for what I believe.
I am going to Indonesia to pilot what I believe is the world’s first system to make doctor work faster while preventing mistakes. The work is premised on a decade of watching stressed-out, overworked, fallible, rare, often not-there doctors, deliver wrong care to patients, resulting in unnecessary intervention, cost, pain and death. Years ago, my teams in Liberia and later Indonesia culled through thousands of dusty paper medical records and measured hospital medical error rates between 50-80%. This error range is astounding but put into perspective, medical errors in the United States approach 20-40% resulting in 100,000-200,000 deaths a year. Medical errors can be defined as harm or potential harm from not doing what is supposed to be done according to existing evidence or established medical practice. Or, it can be harm or potential harm caused by interventions done outside of existing evidence and established medical practice. So you go to a doctor with some diarrhea and they give you antibiotics when they’re not supposed to. You have a reaction to the antibiotics, which gives you a rash that goes away in three days (error of commission). Or you go to a doctor with one month of cough and the doctor tells you its from your smoking and to stop that but it’s really undiagnosed asthma. Later, you have a breathing attack and you die (error of omission). In either case, the treatment decision resulted from medically unacceptable (in front of a jury) behavior that injured the patient or risked injuring the patient.

This situation classifies as a medical error too
Most people are very generous to doctors and try to protect them. They say, wait, how can doctors be perfect to which one could respond, not perfect, only competent, and such may be the life of respected person who is paid $250,000 a year, or equivalent. I have seen tens of newborns literally starved to death in the baby ward because they were too premature to suck sufficiently and ask for milk. The concrete walls of hospitals in too many places echo with the cries and anguish of family members who have lost a loved one because a doctor could not be found or because s/he did not have sufficient experience to do surgery and remain sterile.
My company Walking Doctors (WD) believes that there is no such thing as bad people, just bad systems. But that it is also criminal to continue health practices known to cause harm. Our strategy is simple and not mine-- pretty much used in every technical industry except the Medical industry for decades. The strategy is to present to the clinician, right when they are about to make an diagnostic or treatment decision, a checklist of things to consider, be done and document in case they forgot. Going back to the previous medical error examples, the WD system would tell a doctor NOT to give antibiotics to a patient with non-bloody diarrhea who looks well and who is not vomiting. For a patient with long-time cough, the WD system would ask the doctor to rule out asthma first through lung exam, spirometry, or medication trial (the dose of which will be automatically calculated). It’s not that hard. Workers at McDonalds have a list of customer burger orders before them. Pilots don’t just arrive in the cockpit ten minutes before departure and take off the plane.
That’s the front end-- A system of interactive reminders. But a back-end feedback mechanism is just as vital. Every manager knows that if you don’t provide feedback to people who are working hard, they feel unappreciated and their performance deteriorates. With doctors it is the same. Due to the doctors’ hierarchical position, however, you have to have a way to expand the reach of health outcomes-- to patients, communities, researchers, teachers and leaders-- to elevate and maintain the expectation, pressure and the reality of high performance. So in the WD system, at any point in time, the health facility website will display how many patients have been seen and for what—outputs. But a click will also display percentage of patients who have been treated according to the evidence base and number of deaths or transfers—outcomes. Moreover, the user can compare facility performance and stratify outputs and outcomes over time.
Doctors will fight this. They are scared of being misinterpreted or scared of being interpreted. But the tide is turning, technology has caught up and one should as a rule tackle fears. People indirectly or directly buy medical services, full stop. In the U.S., it’s $3 trillion dollars a year. In Indonesia it’s $27 billion dollars a year. In Liberia it’s 1/4 of all national spending. There is growing acceptance that the public deserves to know the state of its investments. If I am about to have heart surgery I want to know how many surgeries my doctor has done and to what result. I’ll go even go further. I want to know if my doctor was a ‘C’ student and if s/he has cases before the state medical board for tripping on acid during work. My wife calls me extreme.

Checklists in the flow of one's daily routines is called decision support
Checklists and performance reporting must be a part of a professionals daily work, i.e. quality can’t be extraneous to the routines of doctors, pilots, nuclear engineers, even police men. Everyone knows that a doctor must chart. So WD has embedded its checklists and performance dashboards into a best in class electronic health system (EHS). I say best in class EHS because we made this system too! In fairness, we tried to use systems already available in the market but they were too expensive. Also, since they had been built with billing capture as their main objective, they could not be adapted to support quality tools. Also, they were running off 5-year-old technology. Finally, they were static in-facility devices. We needed a system that could link the spectrum of health facilities with networks outside of health care for data sharing and learning.
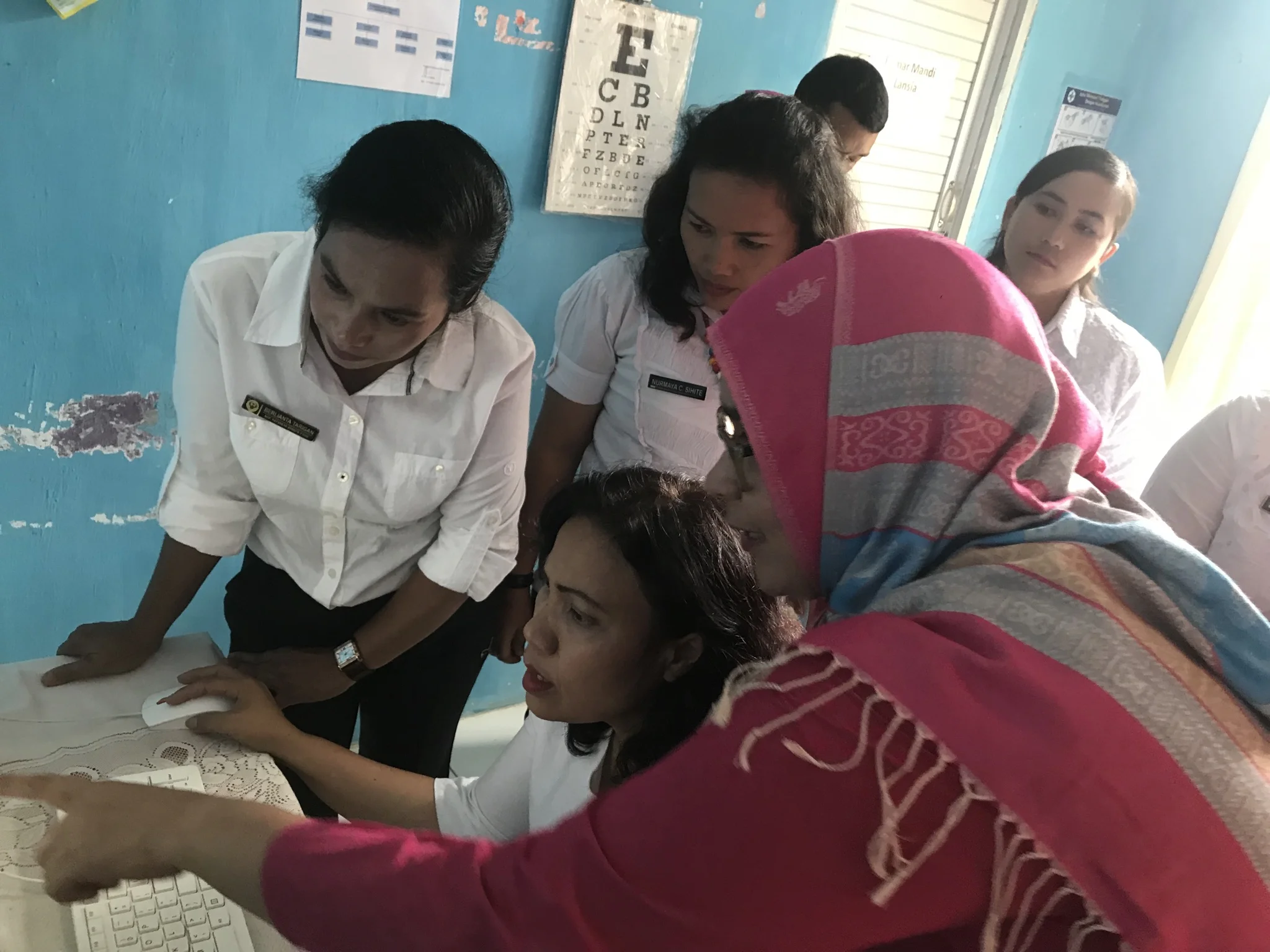
In my last conversation with an advisor who is helping Walking Doctors grow and stabilize as a company to make impact, he warned, to try not working with the government as a customer at first at least on account of its vagaries. He also suggested that we try to ease the barriers of implementing a new device in terms of access to working technology in remote places. Of course, he is exactly right but his advice necessarily emboldened us because Walking Doctor’s first customer is the Governor of Pakpak Bharat, a district of 50,000 people in Northern Sumatra, accessible from the nearest airport only by winding ascending five-hour car ride. (Note to vacationers: Pray your luggage comes). Internet is not ubiquitous here and the medical staff in eight health centers and one hospital have never used electronic medical anything. But the governor or Bupati is famous in Indonesia for having positioned Pakpak Bharat as a hub of technology and higher education. He saw the Walking Doctors product last July when I was in Jakarta. After a one and a half hour presentation and discussion, he asked me if we would consider coming to his district to support the Pakpak Bharat health system. He told me that after a three month pilot in three health centers and one emergency room, if all went well, we could expand to all eight of Pakpak Bharat’s health centers and the entire hospital at which time he would put us in the District budget. This was an offer filled with risk and opportunity. On the risk side: Who was this man? Would our technology work in such a remote place? Would the governor fulfill his promise and hard wire all his health facilities for our electronic health system to run?
But the opportunity to have an entire district to be responsible to and for was unique. If we could succeed in Pakpak Bharat we could succeed anywhere. Where would we find another Bupati, who in Indonesia carries enormous budgetary and policy power, to protect a company with an idea that proposes to fundamentally change medical practice, its impact and its intentions?
My team said what the hell. I said might as well. I don't hear anyone else knocking on our door.
So here we go. Follow us as we go.

Pakpak Bharat's General Hospital and surroundings